Fungi are a group of eukaryotic organisms that present as either a unicellular organism (Yeast) or a multicellular organism (Mold). They are nearly everywhere in nature, but only a small percentage can cause disease in humans. Most of the infections that occur are asymptomatic or so mild that that are not detected. Many of the pathogenic Fungi are dimorphic, meaning that they are present in the form of a mold in colder temperatures and present in the form of yeast at warmer temperatures (such as body temperature after infecting a human). A way to remember this is the mnemonic “Mold in the Cold, Yeast in the Heat.” Fungi have a complex reproductive life cycle that includes formation of Spores which can live in the environment in a vegetative state. Humans usually contract fungal infections by acquiring these spores from environmental sources such as soil. Most fungal infections do not have a person to person spread. Mold form hyphae while Yeast form budding yeast and psuedohyphae. Both hyphae and Psuedohyphae are branching filamentous vegetative structures of fungi and each form spores. True hyphae have septae or cell walls between sections while psuedohyphae are formed by budding without a true cell wall/septae between sections.
Systemic vs. Opportunistic Mycoses:
The high yield fungal infections can primarily be broken down into two groups, Systemic and Opportunistic. Fungi in the systemic category have a higher virulence and can infect health individuals. While these fungi can infect immunocompetent individuals the infections are usually mild and localized to the respiratory system. In immunocompromised individuals the infections can more commonly spread from the lungs and disseminate to the rest of the body. Systemic fungi are found in specific geographic regions so when a question stem mentions a specific state that should be a buzzword to consider these fungi. Opportunistic Fungi are lower virulence and have to “wait for the right opportunity” to infect a host. Opportunistic infections usually only occur in immunocompromised patients such as those with AIDs, transplanted organs, or cancer.
For both Systemic and Opportunistic Mycoses infections the route of infections is most often inhalation of a spore from an environmental source. This first leads to a respiratory infection, and then given the right circumstances the infection may then spread to other parts of the body. Candida is the exception as it is normal skin flora. We all have Candida present on our skin and it only causes a problem when factors lead to an overgrowth of the fungi.
For the most part, these different fungal infections cannot be differentiated based only on the signs and symptoms. Most of the fungi present like pneumonia with vague flu like symptoms. Therefore, the different fungi are primarily differentiated based on histologic examination of the sputum, biopsy or swab. A stain such as PAS or silver stain is usually needed to visualize the fungi. You should be able to identify the histology of each fungus via pictures and text description of the findings as you can be presented with either in the question. Another thing they sometimes put in the question stems is a patient who seems to have bacterial pneumonia, but is not responding to any broad spectrum antibiotics.
Systemic Mycoses:
Here is a map that shows roughly where you can get the different systemic infections in the United States. Note that there is an overlap between Histoplasmosis and Blastomycosis.

Coccidioidomycosis is one of the Systemic Mycoses. It tends to be found in the southwestern part of the US. Question stems for Coccidioidomycosis may also mention a recent earthquake or an occupation such as construction which can help spread spores from soil into the air. “Spherule full of endospores” on sputum culture. Eventually the spherule will rupture releasing the smaller endospores.

Histoplasmosis is another Systemic Mycoses. It is found primarily in the Mississippi and Ohio River Valley. Histoplasmosis questions may make mention of the patient being in caves or cleaning bird cages as it can be found in sole contaminated with bat or bird droppings. On histology “macrophages filled with many ovoid cells” since this fungi is intracellular.

Blastomycosis is also a Systemic Mycoses. It is found east of the Mississippi River and is often associated with exposure to bodies of water like ponds and riverbanks. Histologically it appears as a large yeast with “Broad Based Budding” (Think All Bs).

Opportunistic Mycoses:
Cryptococcus Neoformans is an opportunistic mycoses infection associated with exposure to pigeon droppings. Following inhalation and infection of the respiratory system, Cryptococcus has a predilection for spreading to the meninges and causing Meningitis. Cryptococcus is monomorphic and not present as a mold. Its main virulence factor is an antiphagocytic polysaccharide capsule which can be seen with India Ink stain. Histologically it appears as singular budding yeast with a “halo.”

Aspergillus Fumigatus is an Opportunistic Mycoses with a number of different high yield presentations. Allergic Bronchopulmonary Aspergillosis is when the fungus colonizes the airway of patients with CF or asthma leading to a hypersensitivity reaction. It presents with asthma like symptoms and migratory pulmonary infiltrates. It can be identified with an aspergillus skin test. An Aspergilloma (AKA “Fungus Ball”) is when the fungus fills up a cavitary lung lesions previously formed by a TB infection or other lung injury. Aspergillus is also associated with hepatocellular carcinoma as the fungus produces a carcinogenic Aflatoxin. Histologically presents with “V-shaped” hyphae branching at acute angle (about 45 degrees).

Pneumocystis Jiroveci is an opportunistic infection that primarily presents as Pneumocystis Pneumonia (PCP) in patients with AIDs. PCP usually has diffuse bilateral interstitial infiltrates in patients with CD4 T Cell counts below 200. Once counts are below 200 AIDs patients should be given Trimethoprim/Sulfamethoxazole prophylaxis to prevent PCP. Previously known as Pneumocystis Carinii.
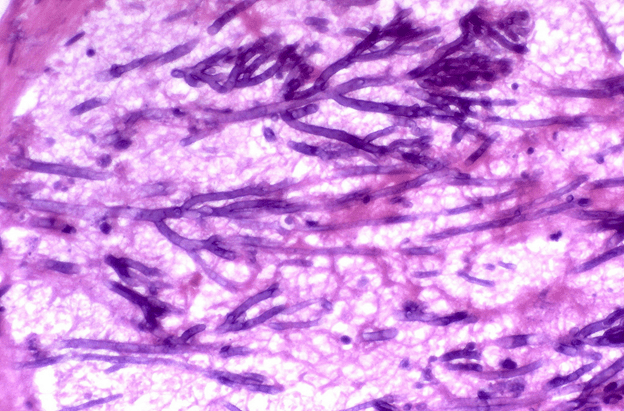
Mucormycosis & Rhizopus (AKA Zygomycosis) are opportunistic mycoses that are usually seen in diabetics (most often during ketoacidosis). It results in an infection of paranasal sinuses or the eye that can extend into the brain. The fungi infect the vessels and can form a clot leading to a necrotic black eschar. Histologically it has “ribbon like” hyphae without septae branching at a wide angle (about 90 degree).

Localized Fungal Infections:
We have already discussed the more serious fungal infections which can spread through the body. Now we will move onto the less serious infections which are localized to the skin, mouth and/or vagina.
Tineae is a group of common fungal infections that are primarily localized to the skin, hair and/or nails. Tinea Versicolor is caused my Malassezia Furfur and leads to well demarcated areas of hyperpigmentation or hypopigmentation. It is more common in young adults especially in hot weather and occurs on the trunk more than other regions. Dermatophytes cause Tinea Corporis (AKA Ringworm), Tinea Pedis (AKA Atheletes Foot), Tinea Capitis (superficial scalp infection) & Tinea Unguium (infection of the nails). Ringworm usually presents as a scaly erythematous circular lesion with central clearing. Tinea Capitus is a scaly area on the scalp which may have localized alopecia (hair loss). Infections of the nails (AKA Onchomychosis) are more commonly in elderly individuals, are very tough to treat and present with thickened opacified nails. Athletes foot is a scaly pruritic erythematous lesion of the feet most common in young adults. Scrapes of these superficial fungal infections can be shown on KOH prep to have a “spaghetti and meatball” pattern of hyphae and yeast balls.


Candida is part of normal skin flora and the most common cause of fungal infection worldwide. It is an opportunistic infection that most often effects the vagina (AKA “Yeast Infection”), mouth/tongue (AKA “Thrush”), and genital area (AKA “Diaper Rash”). However, it can also occur in the esophagus (particularly in HIV patients), between skin folds (primarily in the obese), and heart valve (IV drug users). Infections can arise soon after antibiotic treatment as the removal of “good” bacteria allows for overgrowth of the fungal flora. Histologically it presents with oval budding yeast and psuedohyphae. It forms germ tubes (true hyphae) when incubated at 37 degree Celsius for a few hours.
Sporothrix – seen when spores on a thorn get introduced under the skin by a thorn prick. Question stems usually mention a rose gardener. In immunocompetent individuals it causes a localized subcutaneous nodule and/or an ulcer at the site of skin breakage.
Antifungals:
- Azoles (Fluconazole/Diflucan, Ketoconazole, Miconazole, Itraconazole …) inhibit the cytochrome P450 Lanosterol 14 Alpha Demethylase enzyme which is necessary to convert Lanosterol into ergosterol. Ergosterol is important for fungal function as it acts in the cell membrane similar to cholesterol in our cells. Mutations that encode for the enzyme can prevent the drug from binding to the enzyme and lead to drug resistance. This class of drugs has a wide range of antifungal uses, from serious to mild. Some are even available over the counter.
- Amphotericin B & Nystatin bind to the ergosterol in fungal cell membranes creating pores. Nystatin is most commonly used in the form of “Swish and Swallow” mouthwash for thrush. Amphotericin B is used only for serious systemic fungal infections or fungal meningitis due to its severe side effects (Hence the mnemonic Ampho-terrible). Soon after it is administered Ampho B can cause fever, chills & hypotension (AKA “Shake and Bake”). The drug is also nephrotoxic.
- Capsofungin & Micafungin (AKA Echinocandins) inhibit a glucan synthase enzyme depriving the fungal cell wall of necessary polysaccharides.
Pictures Used:
- “Coccidioidomycosis_Spherule” by CDC available at https://commons.wikimedia.org/wiki/File:Coccidioidomycosis_Spherule.jpg via Public Domain
- ” Histoplasmosis Capsulatum” by CDC available at https://en.wikipedia.org/wiki/Histoplasmosis#/media/File:Histoplasmosis_capsulatum.jpg via Public Domain
- “Blastomyces dermatitidis” by CDC available at https://en.wikipedia.org/wiki/Blastomycosis#/media/File:Blastomyces_dermatitidis_GMS.jpeg via Public Domain
- Derivative of “Blastomycosis cropped” by Joel Mills available at https://commons.wikimedia.org/wiki/File:Blastomycosis_cropped.JPG via Creative Commons 3.0 Attribution-Share Alike
- Derivative of “Cryptococcus neoformans using a light India ink staining” by CDC available at https://commons.wikimedia.org/wiki/File:Cryptococcus_neoformans_using_a_light_India_ink_staining_preparation_PHIL_3771_lores.jpg via Public Domain
- Derivative of “Cryptoccocus Gram Film” by Graham Beards available at https://commons.wikimedia.org/wiki/File:Cryptococcus_Gram_film.jpg via Creative Commons 3.0 Attribution Share Alike
- Derivative of “Aspergilloma complicating tuberculosis 2” by Yale Rosen available at https://commons.wikimedia.org/wiki/File:Aspergilloma_complicating_tuberculosis_2.jpg via Creative Commons 2.0 Attribution-Share Alike
- “Aspergillosis, angioinvasive, intravascular” by Yale Rosen available at https://www.flickr.com/photos/pulmonary_pathology/5390967599 via Creative Commons 2.0 Attribution-Share Alike
- Derivative of “Zygomycosis/mucormycosis” by Yale Rosen available at https://www.flickr.com/photos/pulmonary_pathology/5390897069 via Creative Commons 2.0 Atribution Share Alike
- Derivative of “Zygomycosis, Mucormycosis 1” by Yale Rosen available at https://commons.wikimedia.org/wiki/File:Zygomycosis,_mucormycosis_1.jpg via Creative Commons 2.0 Attribution-Share Alike
- Derivative of “Zygomycosis” by Nephron available at https://commons.wikimedia.org/wiki/File:Zygomycosis.jpg via Creative Commons 3.0 Attribution-Share Alike
- “Ringworm on the arm, or tinea corporis due to Trichophyton mentagrophytes” by CDC available at https://commons.wikimedia.org/wiki/File:Ringworm_on_the_arm,_or_tinea_corporis_due_to_Trichophyton_mentagrophytes_PHIL_2938_lores.jpg via Public Domain
- “Teigne – Tinea capitis” by Grook Da Oger available at https://commons.wikimedia.org/wiki/File:Teigne_-_Tinea_capitis.jpg via Creative Commons 4.0 International Attribution Share Alike License
- “Onychomycosis due to Trychophyton rubrum, right and left great toe” by CDC available at https://commons.wikimedia.org/wiki/File:Onychomycosis_due_to_Trychophyton_rubrum,_right_and_left_great_toe_PHIL_579_lores.jpg via Public Domain
- “Tinea versicolor1” by Sarahrosenau available at https://commons.wikimedia.org/wiki/File:Tinea_versicolor1.jpg via Creative Commons 2.0 Attribution-Share Alike
- “Candida albicans” by Y Tambe available at https://commons.wikimedia.org/wiki/File:Candida_albicans.jpg via Creative Commons 3.0 Unported Attribution-Share Alike License
- “Human tongue infected with oral candidiasis” by James Heilman available at https://commons.wikimedia.org/wiki/File:Human_tongue_infected_with_oral_candidiasis.jpg via Creative Commons 3.0 Unported Attribution-Share Alike
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}